![]()

RHP&EO is the electronic journal of the International
Union for Health Promotion and Education
![]()
|
|
|
Public health associations as key players in influencing public policy[1] By Dior Ba, M.Sc. in policy analysis (candidate), Université Laval and Louise St-Pierre, CCN-PPS/INSPQ and PhD in Community Health (candidate), Université Laval Ba, Dior & Louise St-Pierre, Public health associations as key players in influencing public policy, Reviews of Health Promotion and Education Online, 2007. URL:23/index.htm. The adoption of the Ottawa Charter in 1986 (WHO, 1986) brought to light the strategic significance of developing healthy public policies. Such policies are characterized by an explicit concern for health in all sectors of government jurisdiction (education, transportation, revenue, etc.). Healthy public policies thus promote the creation of a physical and social environment that allows the public to lead a healthy life (Nutbeam, 1998).
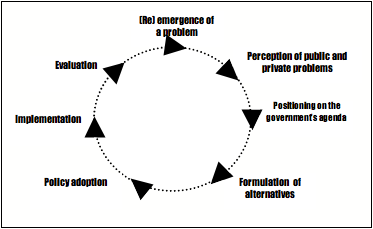
The most recent edition of the Journées annuelles de santé publique provided the opportunity to highlight the 20th anniversary of the Ottawa Charter. The Association pour la santé publique du Québec, together with other Canadian public health associations, took this opportunity to reflect upon their roles as policy actors. The National Collaborating Centre for Healthy Public Policy (NCC-HPP), located at the Institut national de santé publique du Québec (INSPQ), participated in this process by exploring some of these organizations experiences on the basis of concepts borrowed from political science. As participants in this venture, we are pleased to provide here some reflections triggered by that most stimulating workshop. First, we will briefly present the analytical framework used to explore the role of public health associations in the development of healthy public policies. Then, for illustrative purposes, we will present reflections stemming from a literature review and a series of interviews with key informants from three public health associations in Canada: the Association pour la santé publique du Québec, the Public Health Association of British Columbia, and the Canadian Public Health Association. Public policy There are many definitions of public policy in the literature. Generally speaking, we may consider a public policy to be a decision made by a governmental authority with the objective of acting, or not acting, to resolve a problem (Lemieux, 2002; Howlett & Ramesh, 2003; Meny & Thoenig, 1989). A public policy may also be seen as the result of a process involving at least five key phases: i) the emergence of a problem that requires the attention of the public and decision makers, ii) placing this problem on the governments agenda in order to find a solution; iii) the formulation of various alternatives to resolve the problem, iv) the adoption of a policy, and v) the implementation and the evaluation of a policy. Figure 1 illustrates the public policy cycle (Knoepfel, Larrue & Varone, 2001). It must be emphasized that the development of a public policy is not a linear process but rather a iterative one. In the context of the workshop, we were particularly interested in the role of public health associations in putting issues on the agenda, in formulating alternatives and in the adoption of a policy option by a government. Figure 1. The public policy cycle
Adapted from Knoepfel, Larrue & Varone, 2001: p. 37 A number of stakeholders are involved throughout the public policy process. These people attempt to influence, and even control, the decisions, particularly during the emergence, formulation and adoption phases. Thus, the development of public policies is influenced by the dynamics of power among the policy actors. According to Lemieux (2002), we can categorize these players into four groups: private individuals, interested parties, officials and elected people. Within government we find the officials and the elected. The officials are the bureaucrats, the content specialists whereas the elected are formally representing their constituencies and have executive and legislative capacities. Outside of government are the interested parties and private individuals. Interested parties are usually experts, interest groups and other content specialists whereas private individuals refer to the general population directly or indirectly affected by the policy. Public health organizations and individuals may be part of the interested parties or of the private individuals. In fact, they may play the roles of expert and/or of representative of the population. The power held by policy actors varies a great deal and depends on the resources and advantages they are able to use to succeed in their efforts. The position they hold in society (status), their access to information (informational advantage), the control they have over resources (levers of power), their connections with the other stakeholders (relationship advantage), and the values they share with the public (normative advantage) are all potential assets (Lemieux, 2002). Public health organizations usually have several of these assets, notably relationship, informational and normative advantages. They also enjoy a certain status in the public eye, making them stakeholders with potential influence. Getting onto the governments agenda Several political scientists have developed theoretical models to explain why certain issues are placed on the governments agenda and others not. One of the most frequently cited models is that of Kingdon (1995). According to him, for an issue to get on the governments agenda, three streams must converge to create a window of opportunity: the problem, its solutions and the political situation.
Thus, the emergence of a major problem, the existence of a solution, and a favourable political climate constitute important factors in order for a problem to be placed on the governments agenda. Nevertheless, the arrival of a window of opportunity is also usually required for the government to take a problem into consideration. Such a window of opportunity may be predictable (e.g. an election) or unpredictable (e.g. a crisis). Generally speaking, an issue is more likely to be placed on the agenda if there are individuals or groups (called entrepreneurs) who get involved to advance the concepts within the three streams and who are able to combine these streams when a window of opportunity opens. The following table links the main phases of the policy circle with the interactions between the various players, the types of advantages they usually possess and the streams, as described by Lemieux (2002).
Table 1: Streams, players and the use of power advantages*
*Only the elements most relevant to the analysis were considered. Source: Lemieux (2002) Coalitions and subsystem As previously mentioned, policy actors may attempt to influence decision makers to highlight an issue, place it on the governments agenda or define the policy alternatives that should be retained. According to the theory of Sabatier and Jenkins-Smith (1993), a policy is sometimes subjected to lobbying from at least two major coalitions, identified in his model as advocacy coalitions. These coalitions group together individuals and organizations for or against a policy in a close or not so close way, depending upon the issue involved. These coalitions may include, for example, government officials from the lead department and other departments affected, public and private organizations, community groups, researchers and academics, etc. The values and ideas they share bring these players together. They rely on a certain number of beliefs that allow them to define their strategy in order to influence the political decisions to be made. The goal of any coalition is to ensure that the problem, which is already on the governments agenda in some cases, is considered a priority or attracts more attention from the authorities. A coalition may also work in the opposite way, by preventing a problem from being considered a priority on the agenda. The more a coalition shows internal cohesion under strong leadership, the greater its chances of success (Cohn, 2006). Public health associations as political players As policy actors, public health associations get involved particularly in the emergence phase, in order to get a societal concern on the governments agenda. This seemed to be the experience of the three present at the JASP workshop. For example, the Association pour la santé publique du Québec (ASPQ) has been very involved around perinatal issues in Québec. By organizing in the 1980s regional conferences throughout the province named Accoucher ou se faire accoucher ? (give birth or be delivered), the Association greatly contributed to bringing to light the concerns of women regarding the humanization of childbirth. Also, its close links with the Department of Social Affairs (now the Department of Health and Social Services) allowed it to take advantage of a window of opportunity during the revision of the policy on perinatality to propose and strongly support the introduction of midwifery in Quebec. This support was demonstrated by the shaping and leadership of a coalition in support of this innovation, which popularized and distributed scientific information to counterbalance groups favourable to maintaining the then ongoing process of the medicalization of childbirth. The Association was involved in formulating the solution, although certain compromises had to be made. ASPQ played an entrepreneur role in this issue by contributing to placing midwifery practice on the agenda in Quebec, by seeking public support and by mobilizing players in favour of this option. The Association also took advantage of its close relationship with government officials, its relationships with midwife groups and its in-depth knowledge of the issue. As another example, the Public Health Association of British Columbia (PHABC) is currently taking advantage of the window of opportunity presented by the 2010 Olympic Games. This opportunity came along with the British Columbia governments intention to become the Canadian province with the healthiest residents. This provincial government has planned to achieve such a goal before the Olympic Games and has thus proposed a series of cross-sectoral programs in this respect. The PHABC, until now a rather weak player on the political scene, embarked wholeheartedly in this movement. Among other things, the PHABC assumed leadership of a public health group working in food safety, more specifically, nutritionists lobbying for health to be taken into account in the development of food-processing policies. Thanks to this window of opportunity, the PHABC has been able to increase its staff, get additional funding and boost its credibility. It also expects to benefit from these resources and advantages to influence related government policies. By being involved in this way and by rallying other public health organizations on this specific topic, the PHABC aims now at becoming a key political player on any issue relating to population health. It is striving to develop its advantages, its mobilization capacity and its scientific credibility. Finally, the Canadian Public Health Association (CPHA), an old political player on the Canadian health scene, also hopes to continue to expand its mobilization capacity based on its scientific credibility. As an example, a window of opportunity presented itself during the SARS crisis there was a political and collective awareness of the importance of strengthening the public health systems in the provinces. The CPHA assumed leadership of the Canadian Coalition for Public Health in the 21st Century that brought together over 60 organizations from across Canada and, with a strong collective voice, used every possible occasion and forum to bring up this commitment and was surely key in stimulating the creation of the new Public Health Agency of Canada. Over the years, the CPHA has developed important links with the academic community and governmental organizations, making it one of the most significant and credible public health actors in Canada. Building on this credibility and notoriety, it will surely continue to influence and support the adoption of healthy public policies. Conclusion: The valuable assets of public health associations As we have seen in the examples presented above, public health associations can clearly act in each of the streams defined by Kingdon that contribute to getting an issue placed on governments agendas. They can definitely play an entrepreneur role by highlighting key public health issues and by identifying acceptable and relevant solutions. They also have the capacity to mobilize a large number of organizations and individuals who can rally around the values conveyed by the public health community. They have demonstrated their ability to identify and take advantage of windows of opportunity that may advance their causes. Lastly, the nature of their organizations favourably places them at the crossroads of scientists, decision makers and the public, a position that allows them to utilize their specific assets. Considering all of these advantages, our message for the Vancouver conference is clear and will hopefully be discussed there: public health associations can and should play an important role in the development of healthy public policies. By using the analytical tools developed in political science, the public health associations can refine their ability to read the contexts and the stakes associated with public policy processes, and thus expand their capacity for action. [1] The original version of this paper was published in French as : Les associations de santé publique : des acteurs-clés pour influencer les politiques publiques. Bulletin de lAssociation pour la santé publique du Québec. Décembre 2006/ Janvier 2007. It is available from the ASPQ (http://www.aspq.org) upon request.
References Cohn, D. (2006). Jumping into the Political Fray: Academic and Policy-Making. Institute for Research on Public Policy, 7. PDF: http://www.irpp.org/pm/archive/pmvol7no3.pdf Howlett M., & Ramesh M. (2003). Studying public policy: Policy cycles and policy subsystems. (2nd edition). Oxford: Oxford University Press. URL: http://www.oup.com/ca/isbn/0-19-541794-1 Kingdon, J. W. (1995). Agendas, Alternatives and Public Policies. New York: Harper Collins College. Knoepfel, P., Larrue, C., & Varone, F. (2001). Analyse et pilotage des politiques publiques. Bâle, Switzerland: Helbing and Lichtenhahn. Lemieux, V. (2002). Létude des politiques publiques : les acteurs et leur pouvoir (2e édition). Québec: Les presses de lUniversité Laval. URL: http://www.pulaval.com/catalogue/etude-des-politiques-publiques-les-acteurs-3287.html Meny, Y., & Thoenig, J.-C. (1989). Politiques publiques. Paris: Presses universitaires de France. Nutbeam, D. (1998). Health promotion glossary. Health Promotion International, 13, 349-364. PDF: 15/_derived/349.pdf Sabatier, P. A., & Jenkins-Smith, H. C. (1993). Policy Change and Learning: An Advocacy Coalition Approach. Boulder, CO: Westview. URL: http://www.perseusbooksgroup.com/westview/book_detail.jsp?isbn=0813316499 World Health Organization. (1986). Ottawa Charter for Health Promotion. Geneva: World Health Organization, Health and Welfare Canada, Canadian Public Health Association. URL: http://creepublichealth.org/public/files/CBHSSJB%20Sectoral%20Report%20Volume%202.pdf | |||||||||||||||||
|
|